JPSTSS Report of the Sixth European Surgery Tour
・・・・・・Kosei Nagata,M.D. Orthopedic dept. University of Tokyo・・・・・・
Dr. Yusuke Sato had already reported the details of the sixth European surgical tour, and I am going to report in detail the operation performed by Dr Sebastien Charosky in the Center Toulousain Rachis, Polyclinique du Parc.
A 58-year-old woman had low back pain for 2 years. She presented to the hospital in 2016, and her standing sagittal radiograph showed a moderate lumbar lordosis and instability in L3/L4, L4/L5, and L5/S (figure 1 and 2).
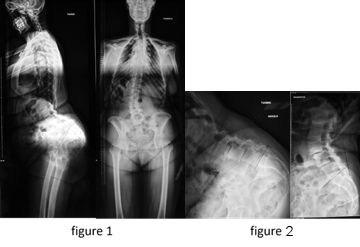
Her pelvic incidence (PI) angle was >90° based on the morphology of the pelvis. Computed tomography revealed lumbar spinal canal stenosis and disk degeneration. In February 2016, she underwent posterolateral fixation from Th12 to the sacrum. In addition, a three-level interbody fusion was performed, and >70° of lumbar lordosis (LL) was gained in March 2016 (figure 3).

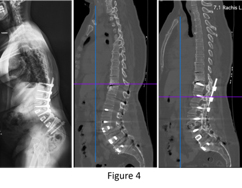
However, 10 months subsequent to the initial operation, the patient developed an upper back pain at the Th11/Th12 level. Proximal junctional kyphosis (PJK) was observed on the CT scan, although interbody fusion was also observed and L3-to-sacrum fixation was performed (figure 4).
He diagnosed the patient as having PJK due to PI-LL mismatch and planned extension of the fixation, and pedicle subtraction osteotomy (PSO) at L5 was planned to attain a large LL. He chose Th3 as the uppermost instrumented vertebra in the revision surgery to make an ideal thoracic kyphosis (TK). We were introduced to observe the revision surgery in September 2018.
Dr. Charosky has always performed surgery single-handedly and very quickly. To shorten the surgical time, thoracic fixation was performed by skipping like right T3 hook, left T4, right T5, and left T6 pedicle screw owing to physiological stability of the thoracic vertebra. The rods were bended and connected to each pedicle screw or hook by using lateral connectors in consideration of the harmonic TK. The third rod was added to increase the posterior stability (figure 5).

Dr. Charosky emphasised the non-touch technique; surgeons should not touch the operative field with gloves for infection control. The operation time was around 4.5 hours.
In January 2019, 4 months after the surgery, Dr. Charosky presented us the consecutive images and reported that the patient began to show progressive relief of her thoracic back pain and that the instrument was stable. The TK was 45° and LL was >90° in this patient; therefore, the PI-LL was modified into within 10° (figure 6).

This operation consisted of two important points. First, the revision surgery with L5 osteotomy was technically challenging. Second, a large PI angle, especially >80° was reported to be rare. The mean PI angle of Japanese female volunteers between 50 and 59 years of age was approximately 50° in the Wakayama Spine Study. A moderate correlation (0.3 < r < 0.5) was observed between TK and LL. Here, we thanked Dr. Charosky for inviting our tour and have to emphasise his sophisticated techniques.
●Reference Data【Original images Dr.Charosky(pdf:1MB)】
|










